
The CCN Regional Trauma-Informed Care (RTIC) Pilot Implementation Framework Program was created by a team of 21 dedicated and passionate individuals from colleges, county government, health care, social care, human services, and schools spanning across Care Compass Network’s 9-county region. Prior to the team’s formation, entities were working independently to advance awareness of Adverse Childhood Experiences (ACEs), trauma and their impact. Meetings took place in separate organizations but actions were not materializing. The work was fragmented without a driving mission or vision for the future. Recognizing the critical need and value to create and operationalize a manageable Trauma-Informed Care Implementation Framework, the RTIC team was formed April 2019.
The intent was to establish an action-based task force, working together to have a direct and positive impact on the community. The group saw value in the implementation and adoption of trauma-informed care principles, believing that practicing trauma-informed care takes into account a holistic person-centered approach, helping to break the cycle of negative impact caused by trauma.
The RTIC team envisioned a resilient community built upon strong partnerships, trust, and compassion and made it their mission to advance the implementation of evidenced-based, trauma-informed care practices by supporting the development of resilient and strong partnerships, individuals, families, and communities through advocacy, education, and empowerment. A core strategy to bring this to fruition was to create and promote access, availability of training, educational tools, and resources for our community.
Report Overview
The following report contains lessons learned, transformations, successes, and case studies highlighting four organizations that participated in the RTIC pilot Implementation framework program from April 2021 to April 2022. Their stories detail the collaboration, commitment, and intentionality demonstrated in order to transform their school, healthcare setting, and community organizations into trauma-sensitive environments for their staff and individuals served.
Each pilot site was assigned a dedicated Care Compass Network Project Manager to support the day-to-day implementation efforts with oversight and assistance from the RTIC Program Director. All four pilots followed the RTIC Pilot Implementation Framework which outlined the required milestones, steps, and deliverables such as specific training was utilized and validated screening tools were implemented. Dialogue among staff and the Core Implementation Team (CIT) was critical in the success of each pilot site.
It is the hope of the RTIC team that lessons learned, successes, and concrete transformations from this collaboration and the collective meaningful experiences of the pilot program participants, more organizations, schools, and healthcare teams will be encouraged to create and cultivate a trauma-sensitive environment of their own.
Executive Summary
ACEs (Adverse Childhood Experiences) and/or traumas does not discriminate. Being employed in the healthcare and helping profession sector significantly places you at a higher risk of experiencing burnout, secondary trauma, and compassion fatigue. Research has shown that helping professionals with pre-exiting anxiety disorders, mood disorders, or personal trauma histories are more susceptible to experiencing Secondary Traumatic Stress (STS), Vicarious Trauma, Compassion Fatigue, and Burnout as reported in Trauma and the Wounded Helper. Coupled that with our shared collective trauma with the COVID-19 pandemic, our community, children, and families were negatively impacted from multiple fronts including physically, socially, emotionally, economically, and educationally.
The National Academy of Medicine (NAM) called on health care leaders to focus on the following core organizational factors as reported in their 2019’s Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-being. As a regional network team, we believe the below call to actions are also applicable/tailorable to community-based sectors and educational settings.
-
- Excessive workload, administrative burden, and bureaucracy.
- Diminished professional relationships, trust, resources, autonomy and engagement, workplace safety and inclusion, and professional development.
- Ineffective compensation and reimbursement structures, performance policies and recognition processes, leadership and mentorship, team functionality, and EHR systems.
Equipped with data, science, support, and a desire to make a difference, the Care Compass Network RTIC Team developed a Trauma-Informed Care Implementation Framework to integrate Trauma-Informed Care (TIC) approaches and practices into the daily operations, with the goal of cultivating a compassionate and safe environment to promote healing, resiliency, and wellness for employees, individuals served, and the community.
Our RTIC trauma-informed care Implementation Framework pilot was a game changer. By flipping the typical narrative of “If we do this, it will improve clients/patients/students’ lives and increase their satisfaction” to “If we do this, we will create a kinder and more compassionate workplace environment to support our staff’s health, resilience, and well-being” so that our staff feel cared for and that our cups are filled and replenished as we continue to care for everyone around us has truly activated and validated the staff’s concerns, needs, and voices.
In an 11–12-month timeframe, our four Regional Trauma-Informed Care pilots were able to achieve and realize the benefits and values of the 4 core TIC priorities and more. Below is a summation of some of the organizational impacts and transformations that were captured and reported as part of the RTIC implementation program final self-reports, data evaluation, and milestones management.
-
- Train all pilot staff on TIC, ACEs, trauma, and its impact on health and wellness.
- Adopt and implement effective and validated trauma screenings, interventions, and follow-up care processes.
- Collaborate and strengthen referral and treatment networks to address trauma and support healing and engagement.
- Implement TIC approaches that advance healing, health and resiliency as well as wellness programs for pilot site staff and patients served.
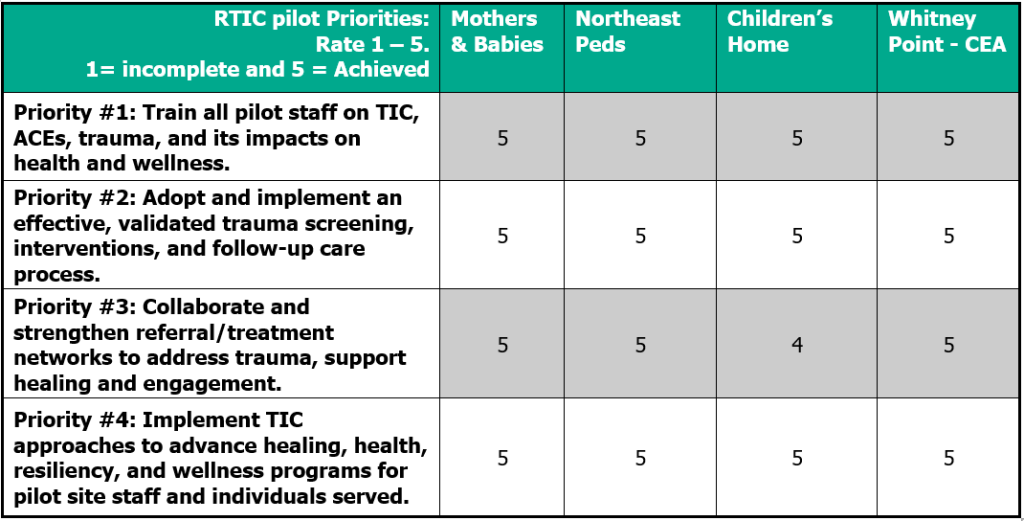
Overall Summary of Organizational Impacts and Results
Our Care Compass Network Regional Trauma-Informed Care Implementation Framework’s 4 core priorities are listed below with each respective pilot awardee’s self-rating on how they felt their pilot site achieved it objectives based on the associated milestones, steps, and deliverables. These self-rating were conducted after the April 31, 2022 project performance period and is based on both the adjudicated milestones completions, qualitative data (observable/shareable stories), final pilot reports, RTIC project manager, and RTIC program director’s assessments. It is worth noting that the only reported score of 4 vs. a 5 was simply the understanding that there is always room for improvement when it came to how we can work to support and strengthen our networks and individuals served.
-
- Train all pilot staff on TIC, ACEs, trauma, and its impact on health and wellness.
- Adopt and implement effective and validated trauma screenings, interventions, and follow-up care processes.
- Collaborate and strengthen referral and treatment networks to address trauma and support healing and engagement.
- Implement TIC approaches that advance healing, health and resiliency as well as wellness programs for pilot site staff and patients served.
Through the RTIC Implementation Framework Milestones and requirements, each pilot was able to apply the SAMHSA (six principles of Trauma-Informed Approach to transform and support their staff, operations, and workplace.
Approach: RTIC Pilot Selection Framework
With the support and funding approval from the Care Compass Network (CCN) leadership team and Board of Directors, the CCN Regional Trauma-Informed Care (RTIC) team identified committed network partners from across multiple settings as potential Trauma-Informed Care (TIC) pilot applicants. The RTIC team reviewed and vetted multiple settings that would provide the most comprehensive approach, benefit, and value in which to learn. As a team, the focus was narrowed down to focus on three key settings; community-based, school-based, and primary care (pediatric, internal medicine, family practice).
Once the initial application outreach framework was finalized, the RTIC team utilized our diverse knowledge and existing relationships to generate a list of potential participants from across CCN’s 9-county service area. The New York State Delivery System Reform Incentive Payment (DSRIP) partners, who participated in many of the transformative projects, were also utilized to provide a comprehensive and holistic analysis to maximize and optimize the pilot selection process. This enhanced selection process was essential as the pilot sites were required to launch by April/May 2021. It became more critical and intentional for the team to evaluate and understand the pilot site’s ability and capacity to carry out the RTIC Implementation Framework milestones. These core concepts and needs were included in the application requirements and scoring framework.
Once a list of potential organizations was obtained, the RTIC Pilot Implementation Framework Program documents were distributed. These documents articulated the purpose of the pilot program, milestones framework requirements, pilot funding, timelines, and deadline for applications. A core requirement was for all potential pilot applicants to thoroughly read, understand, and evaluate their organization’s capacity and availability of their staff to support the implementation efforts on day 1. Each application was explicitly evaluated and scored on alignment of TIC with their overall strategy, mission, and vision. Those with the highest score were selected to move forward.
RTIC Trauma-Informed Care Pilot Implementation Framework Partner Awards
RTIC Phase I: School-based pilot review and selection was completed in March of 2021. The Children’s Home of Wyoming Conference and Whitney Point Central School District’s Caryl E. Adams Elementary were awarded the Regional Trauma-Informed Care (RTIC) pilot funding after a highly competitive review process. Both awardees engaged in the pilot implementation process which began on April 1, 2021.
RTIC Phase II: Community-based and Primary Care pilot review and selection were completed in April of 2021, Mothers & Babies Perinatal Network of South Central New York and Northeast Pediatrics & Adolescent Medicine were awarded the Regional Trauma-Informed Care (RTIC) pilot funding after a highly competitive review process. Both awardees engaged in the pilot implementation process which began on May 1, 2021.
Methodology: RTIC Trauma-Informed Care Implementation Framework Pilot Program
Our RTIC trauma-informed care Implementation Framework pilot is a game changer. We are flipping the typical narrative of “If we do this, it will improve clients/patients/students’ lives and increase their satisfaction” to “If we do this, we will create a kinder and more compassionate workplace environment to support our staff’s health, resilience, and well-being” so that our staff feel cared for and that our cups are filled and replenished as we continue to care for everyone around us.
As defined in the Trauma-Informed Care (traumapolicy.org), Trauma-informed care is a universal framework that any organization can implement to build a culture that acknowledges and anticipates that many people we serve or interact with have histories of trauma and that the environment and interpersonal interactions within an organization can exacerbate the physical, mental, and behavioral manifestations of trauma.
To support the four RTIC pilot implementation, the framework is made up of 7 milestones. Each milestone contains required steps and tasks, which you will find in more detail within the CCN Trauma-Informed Care Implementation Framework for Primary Care and Community-Based toolkits.
These milestones were utilized to lead and support the four RTIC pilots’ transformational efforts. As part of the RTIC pilot grant award, each milestone was allocated a dollar amount with a maximum total earning potential up to $30,000 for each pilot awardee.
Pilot Implementation Framework Overview
In March/April 2021, The Children’s Home of Wyoming, Whitney Point Central School District Caryl E. Adams Elementary, Northeast Pediatrics & Adolescent Medicine, and Mothers & Babies of South Central New York were awarded the RTIC Trauma-Informed Care Pilot after a highly competitive review process and began developing a strategy to implement the pilot framework a few months later in April/May 2021.
The first step for each of the four RTIC pilot was an RTIC pilot kick-off meeting with the Care Compass Network RTIC Program Director and RTIC Project Manager. The agenda included a meet and greet, pilot program overview, project workplan, reporting, resources, and funding requirements. Each RTIC pilot was also assigned a Care Compass Network RTIC project Manager to manage and support the implementation efforts with oversight from the RTIC program director.
The Pilot CIT team reviewed the implementation framework (project workplan) which served as their implementation guide and resources such as how to create a CIT, Project Charter, P-D-S-A cycle, Action Planning, staffing/client baseline, conducting an initial organizational assessment, evaluating and incorporating staff trainings, integrating TIC practices into their policies and procedures, adopting and integrating screenings and interventions into their daily workflow, staff wellness activities and programs, and operation enhancements, and TIC practices into their hiring, onboarding, and retention practices.
For example, as part of Milestone 1, each of the pilot site assembled their Core Implementation Team (CIT) consisting of five to six internal team members who would be leading the TIC implementation efforts at the ground level. Forming the team was part of the first milestone as well as identifying TIC Pilot Champions, Project Sponsors. Once the CIT has been formed, they were tasked with completing an initial organizational self-assessment with their staff and the project charter which required the team to formulate their TIC vision, mission, and action plans (e.g, What does a TIC approach and transformation would look like?).
RTIC Pilot Case Study: Northeast Pediatrics & Adolescent Medicine
In March 2021, Northeast Pediatrics & Adolescent Medicine (Northeast Peds) was awarded the RTIC Trauma-Informed Care Pilot after a highly competitive review process and began developing a strategy to implement the pilot processes and program a few months later in May 2021.
Northeast Pediatrics and Adolescent Medicine is a pediatric primary care private practice with Patient Centered Medical Home (PCMH) recognition by the National Committee for Quality Assurance (NCQA). The PCMH model values team-based care, communication, and coordination with the goal of providing comprehensive, culturally effective patient care to promote positive patient and staff experiences and satisfaction. Northeast Pediatrics cares for about 10,000 patients ages 0-21 from Tompkins, Cayuga, Tioga, Chemung, Cortland, Seneca, and Schuyler counties across their two pediatric locations (Graham Road and Trumansburg Road) and are supported by a team of 44 with a total of 12 providers who are passionate about providing children with exceptional, evidence-based healthcare in a comfortable and welcoming family-centered environment. To further strengthen our patients and families, the team is supported by two full-time Behavioral Health Consultants (BHCs) who works in collaboration with the healthcare providers to provide holistic social, emotional and behavioral care.
Northeast Peds committed to the Trauma-Informed approach because the policies and practices support their collaborative work aimed at fostering a resilient and safe workplace for their staff while providing holistic social, emotional and behavioral care to their patients. They recognized the impact of Adverse Childhood Experiences (ACEs) and made it a priority for all members of their team to feel supported, welcomed and safe in their work environment. The practice further extended this priority to all patients and their families. The RTIC Northeast Peds pilot Core Implementation team (CIT) consisted of seven diverse professionals, including a TIC Pediatrician Champion, TIC Champion, practice administrator, physician assistant, registered nurse, front office representative, and the RTIC Sr. Project Manager from Care Compass Network.
The Northeast Peds CIT was provided an RTIC Trauma Informed Care implementation framework that consisted of five milestones with established steps and deliverables with the goal of integrating TIC practices into their operations, policies, and in doing so, develop new and strengthen existing partnerships with community and clinical resources. These milestones were aimed at achieving a desired outcome of providing TIC support for all staff and patients. In order to achieve this, and subsequent milestones, the RTIC team provided a toolkit Fostering Resilience (thenationalcouncil.org) to assist with the implementation guide along with the RTIC Implementation Framework.
Lessons Learned
Throughout the planning and implementation process, the team at Northeast Pediatrics were faced with many challenges and barriers, one of which was implementing a TIC pilot program during the middle of the COVID-19 pandemic. They had to manage increased demand for sick patient appointments, COVID and flu vaccine roll-outs and changing schedules with staff illnesses and turn-over. Figuring out the logistics for creating physical space conducive for training in a COVID-safe manner, was also a challenge to work through. Despite taking on the pilot project during a pandemic, the team reflected back and recognized how critical and essential the incorporation of this project was to their work, to their staff, and to the patients they served.
The pandemic reminded them that it’s important to be flexible with self-care plans for staff in order to avoid burnout and compassion fatigue. They also recognized that it can be difficult at times to provide time and consideration to gather input from all staff, it is critical to when incorporating new programs and workflows to include input from everyone involved. Northeast Pediatrics that some of their staff had higher ACEs scores than anticipated and staff with those lived experiences desired to be more involved and provide input. As a result, Northeast Pediatrics is intentional with how they listen and respond not only to the people they serve, but also with each other.
As the team at Northeast Pediatrics preserved through these challenging times, the team realized many successes:
-
- Created a calming and interactive outdoor space for staff, families, and patients to enjoy (picnic tables, lawn games, Adirondack chairs).
- Heightened trauma awareness among staff when connecting with their patients and with each other.
- Embedded Pediatric Traumatic Stress Screen Tool (PTSST) screening and surveillance into EMR for annual physicals and well visits.
- Contract for Employee Assistance Program effective 08.01.2021; improved access to mental health services and expanded physical health.
- Increased happiness and loyalty among the staff at Northeast Pediatrics due to the improved health and wellness benefits.
- Improved and expanded evidence-based treatment: two Behavioral Health Consultants (BHCs) are now certified in Trauma Focused-Cognitive Behavior Therapy (TF-CBT).
- Created a new calming staff lounge with comfortable furniture, yoga mats, and mindfulness activities for staff to use.
- Offered staff virtual mindfulness and self-care sessions with our local EAP provider.
- Assisted with gaining an NCQA PCMH Behavioral Health Integration Certification.
- Assisted in meeting some of Value Based Care (VBC) requirements for our insurance companies.
- Strengthened relationships with Project TEACH psychiatrists and psychologists.
The staff have engaged in additional trainings to learn how to understand and care for patients in a way that also prioritizes their needs as well as those of their patients. We are normalizing the conversation across our clinic especially about mental health and self-care. More staff are inquiring about EAP services and resources. Some have expressed feelings of burnout and stress which was helpful and important since being aware and recognizing the signs, symptoms, and triggers is the first step to getting help and support. This mindset shift can be attributed to the RTIC pilot’s trainings and implementation which has allowed us to expand and invest in our staff’s health and wellness programs.
Unexpected Outcomes
The Northeast Peds CIT engaged with their providers and clinical team to ensure early buy-in and support for the trauma screening implementation. At their monthly Provider Journal Club, providers embarked on discussions and reviewed multiple trauma screening tools, studies, benefits, risks, and values to the patient and their families. All of the clinicians were part of the process and provided their recommendations on the selected tool. After much consideration, the team selected the Pediatric Traumatic Stress Screening Tool (PTSST) and incorporated key considerations from the Care Process Module (CPM) for Pediatric Traumatic Stress as part of their policy, procedure. and responses. The clinicians and staff embraced the adoption of a screening tool as a direct result of participating in Milestone 2: Trauma and Competency.
In summary, the RTIC Pilot program has made a difference in the daily practice at Northeast Pediatrics and Adolescent Medicine. The staff trainings and introduction of a universal trauma screening tool has compassion more at the forethought of our minds. Across the office, there are more discussions about the contexts in which our families find themselves rather than being focused on their in-office behaviors as what was prior to the RTIC pilot trainings. With the introduction of the Employee Assistance Program, there are more staff discussing their own therapy and encouraging others to make use of the benefit thus normalizing mental health and getting help. From onboarding, provider time off, to our break spaces, the project has touched every part of the office and work experience. The impact on the staff at Northeast Pediatrics has been instrumental in our ability to create a kinder, safer, and welcoming environment for both staff and patients.
RTIC Pilot Case Study: Whitney Point Caryl E. Adams Primary School
In March 2021, Whitney Point Central School District Caryl E. Adams Primary School was awarded the RTIC Trauma-Informed Care Pilot after a highly competitive review process and began implementing the pilot framework and program in April 2021.
Caryl E. Adams Primary School (CEA) consists of 90 staff members supporting the learning and education for 482 students enrolled in Pre-kindergarten through 3rd grade. The school community is committed to high performance, morale and involvement. The school district identified Trauma-Informed Care (TIC) as a priority for CEA, because it aligned with their vision for achieving a holistic and healthy school community, and because many of their community members and staff have been impacted by trauma. They saw TIC as a way to facilitate learning while supporting the whole student, thereby tending to the social-emotional needs, especially during the COVID-19 pandemic. The staff welcomed the opportunity to develop a common language around TIC, utilizing tools and procedures to support and empower one another so that they can, as a team, effectively support each other and their students, families and caregivers. The staff also acknowledged how TIC helps address the social and emotional needs of the students, including the need to feel safe. Feeling safe is a basic need that must be met before academic, social, and emotional growth can happen.
The Core Implementation Team (CIT) collaborated on a trauma-informed vision which helped to identify what actual transformations would look like as they embarked on their TIC journey.
- Creating a systematic shift in their work as a community school by viewing all of their efforts, including Incredible Years and wellness through a trauma-informed lens.
- Expanding supportive trauma-informed resources for students, families, and staff.
- Standardizing their approach to TIC by working as a team to increase awareness, identify training needs, develop procedures, and implement classroom strategies that address the impacts of trauma.
- Transforming existing student intervention protocol into a standardized and formal closed-loop system of care that includes referral to services.
- Achieving transparency through standardized communication to everyone knows what to expect in different situations.
Lessons Learned
Throughout the planning and implementation process, the CIT team were faced with many challenges and barriers, one of which was implementing a TIC pilot program during the middle of the COVID-19 pandemic and in the month of April during a school year. Despite taking on the pilot project during a pandemic and not starting at the beginning of the school year, the team reflected back and recognized how critical and essential the incorporation of this project was to their work, to their staff, and to the students and families they served.
The pandemic reminded them that it’s more important now than ever to promote and support staff, students, and classrooms with wellness practices and SEL curriculums. Through the RTIC program, trainings and resources, the CEA CIT recognized the value of a restorative culture of care and the healing effects it can have on a school community. They understood how the implementation of specific policies and procedures that create an awareness around trauma, can improve the overall culture within the school. Knowing that these systems are in place, it created an understanding that support is always there and as a result, relationships are built and fostered. Students and staff felt safer and potentially stressful and toxic situations were managed, responded, and resolved in a trauma sensitive approach.
The CEA CIT experienced many successes including a new understanding of the importance of trauma-informed approaches, resulting in more staff reaching out for assistance. The RTIC pilot’s weekly team touchpoint allowed the CIT to explore and understand each member’s role and how they can work together more cohesively as a team. This team building has cemented the CEA Care Team’s ability to collectively address and meet the needs of the staff, students, families, and communities as a whole. Team members also commented on the number of children using the calming strategies taught in the SEL curriculum as a significant and positive outcome.
As the CEA CIT preserved through these challenging times, the team realized many successes:
-
- Helped us to fulfilled the New York State Education Department standards for Social Emotional Learning (SEL).
- Heightened trauma awareness and TIC approaches among staff when connecting with peers, students and families.
- Rebranding of the PPS team to the CEA Care Team to accurately reflect and recognized our services and support that we offered and provide.
- Incorporated TIC education in our onboarding and professional development which will help to streamline the expansion of TIC into our middle and high school as a long-term goal.
- Integrated 7 units of our SEL curriculum via the Incredible Years Dinosaur, into our daily classroom activities, focusing on learning school rules and how to be successful in school; emotional literacy, empathy, perspective taking, interpersonal problem solving, anger management, friendship, and communication skills.
- Incorporated Staff & Student Wellness Activities: Water Bell Challenge, Yoga, Personal Finance, art, GoNoodle® for movement breaks and Calm for meditation breaks in classrooms.
The staff and CIT have gained a heightened awareness around TIC, compassionate fatigue, secondary and vicarious trauma and how it can develop in caregivers. Some staff have shared how the trainings have helped them evaluate their own stressors, triggers, and how their own personal trauma affects them personally and professionally. For these reasons, keeping staff emotionally healthy and well is seen as a high priority, supporting one another and thereby reducing staff and students’ stress and stressful behaviors. As our work progressed, it is important to note that staff might and will still feel a certain level of stress, but now they feel supported and able to talk about what is making them feel overwhelmed. Their awareness of their own trauma, personal triggers, and TIC practices has led them be more in-tune with what might be influencing certain student behaviors.
Unexpected Outcomes
As a result of the RTIC Pilot planning phase, one of the most profound realizations were that many of the faculty and staff were largely unaware of the CEA Care Team’s roles, processes, procedures, and work. Knowing this information, our team became more intentional in the communicating and sharing of our team’s work. Now, our CEA staff has a better understanding of the referral process for students who may be experiencing a social-emotional challenges, including how to refer to the CEA Care Team. The evolution of the CEA Care Team handbook into an ACEs PEARLS screening policy and procedure has helped us to better document and articulate our tiered intervention systems of support.
There are areas in our school that did need attention and improvement, especially around stress. We have been able to address and bring forth trainings, workshops and wellness activities to better support our staff and team.
In summary, this pilot has led to an understanding that there is a real commitment to the well-being of all in the community. The district as a whole has started to recognize that trauma-informed care principles are complementary to the district mission and vision, as evidenced by our recent TRUST-S self-assessment results, where we saw a net 20% improvement across categories. Staff seems to feel more supported by administration as there is an acknowledgment of the stressors, we are under due to the impact COVID 19 has had on our students and society as a whole. Our faculty and staff have a better understanding of our CEA Care Team referral process which they have been using more than ever. There is an overall feeling of safety developed around sharing that one feels overwhelmed or in need of support in her/his/their role. An affirmation shared by Molly Goosman, CEA School Principal, that we did transform our space is when “student teachers and staff who come in as subs from other buildings and schools tell me that they love the supportive climate and want to be here more. They say that it is a profoundly different climate and it draws them in.”
RTIC Pilot Case Study: The Children’s Home of Wyoming Conference
In March 2021, the Children’s Home of Wyoming Conference was awarded the RTIC Trauma-Informed Care Pilot after a highly competitive review process and began implementing the pilot framework and program in April 2021-April 2022.
The Children’s Home of Wyoming Conference (CHOWC) Schools are part of the NYS 853 Coalition – private schools licensed by New York that serve students with a wide range of disabilities in a residential and day school setting since 1985. Our students come from a wide range of counties and present with emotional, social, and behavioral challenges that greatly impact their academic performance and overall success within the school environment. Our Trauma-Informed Care pilot is specific to one section of the CHOWC Schools – the Kresge Middle School. We decided to focus our effort on this area first, to hone in our skills and work closely with students that have been greatly affected by trauma. Our intention is to expand to the Galloway Elementary School and the Kresge High School in September of 2022.
Our pilot Core Implementation team (CIT) consists of administrators, social workers, teachers, and teacher aides. We designed it this way to ensure every level of professional in the school has a voice in the process. The Core Implementation Team (CIT) collaborated on a trauma-informed vision which helped to identify what actual transformations would look like as they embarked on their TIC journey.
Lessons Learned
Throughout the planning and implementation process, the CIT team were faced with many challenges and barriers, one of which was implementing a TIC pilot program during the middle of the COVID-19 pandemic and in the month of April during a school year. Despite taking on the pilot project during a pandemic and not starting at the most optimal time (the beginning of the school year), the team reflected back and recognized how critical and essential this project was to their work, to their staff, and to the students and families they served. The CHOWC CIT were able to complete their TIC trainings within the first few months of the pilot.
The pandemic reminded them that it’s more important now than ever to promote and support staff, students, and classrooms with wellness practices and SEL curriculums such as the SSET to further strengthen their staff’s ability to support their students and families.
Through the RTIC program, trainings and resources, the CHOWC CIT were able to enhanced their school code of conduct and dress code. The RTIC CIT provided trauma-informed language recommendations and/or removal of sections that may not be applicable. The recommendations were warm-handoff to the PBIS (Positive Behavioral Interventions and Supports) team for their input and addition pf PBIS inclusive language with the final goal of presenting to the School Administration for the final review and approval of the code of conduct.
A result, they experienced many successes including a new understanding of the importance of trauma-informed approaches, resulting in more staff engagement, participation and reaching out for assistance. The CHOWC CIT also achieved their RTIC pilot two metrics which aligned with their agency’s 2019-2022 strategic plan. After the completion of the RTIC pilot program, data were analyzed and reviewed:
- 85% Reduction in Restraints:
- 85% decrease between the first 6 months (April-Sept) and the final 6 months (Oct-Mar) of the pilot program. Of all the restraints that occurred during those twelve months, only 13% were from the pilot area students.
- 62% Decrease in staff turnover:
- 62% decrease from the average turnover rate prior to the beginning of the pilot. Of all the staff turnover during those twelve months, only one staff that left the agency was part of the pilot program.
As the CHOWC CIT preserved through these challenging times, the team realized many successes:
-
- Physical Environment Transformations: calming, inclusive and sensory classrooms to help students navigate emotions throughout the day.
- Every meeting begins with a mindful, CARE, and/or TIC moment.
- Heightened trauma awareness of own triggers and using TIC approaches among staff when connecting/advocating with peers, students and families.
- Expansion and enhancement to Employee Assistance Program (EAP) and resources.
- Created TIC playlists to support implementation and learnings.
- Incorporated CANS and ACEs screening within the first 30 day of student admission.
- Reduced membership fees for community and wellness program.
- Incorporated Action Planning for all new initiatives.
- Incorporated TIC and resilience trainings for new staff onboarding.
- Created monthly wellness calendar with activities to promote wellness
The Trauma-Informed Care Pilot has set the tone for how all interactions occur within the pilot area staff. The entire vibe of the pilot area is completely different compared to the areas in our schools that are not part of the pilot.
-
- Staff have gained a heightened awareness around TIC, compassionate fatigue, secondary and vicarious trauma and how it can develop in caregivers.
- Staff are much more supportive of one another, work as a stronger cohesive team, and recognize much quicker that a crisis situation is not about them and is instead about the current experiences of the youth.
- Staff are more receptive to having discussions and hearing about others’ perspectives.
We firmly believe these staff changes are due to the increased knowledge of trauma informed practices.
Unexpected Outcomes
As a result of the RTIC Pilot, we have been able to put a greater focus on staff’s wellness, secondary trauma, and stress, traumas, and how to best support them since it was evident that staff were burnout and experiencing the residual effects of working in a high stress environment. This focus has provided our staff the opportunity to:
-
- Openly share without judgement
- Feel heard
- Gain support from leaders and coworkers
- Understand the impacts of secondary trauma and how it affects their personal and professional lives
The CIT and leaders also noted that supervision with teachers have increased as a result of the pilot. Staff are seeking support beyond the regular schedules instead of avoiding tough conversations. Furthermore, staff are supporting each other in big and small ways every day. There is more receptiveness to feedback and embracing a growth mindset among our pilot staff.
One example of senior administration’s acknowledgement and validation of staff’s need for wellness was the approval of 50% discount membership to the Southern Tier Community Center for all staff members and their families. Completed as part of the CIT’s wellness action plan, the staff truly felt heard and validated in their ask. Currently, the pilot site staffs at CHOWC practice various daily wellness activities throughout the school day which includes meditation, mindfulness, and sensory activities.
As a result of the RTIC pilot and to sustain staff wellness practices, the Children’s Home of Wyoming Conference worked with their EAP company to create a comprehensive presentation on existing and new mental health and wellness benefits for their staff and their families which was delivered to all their staff across the agency. One of the realizations was that many staff were unaware of the many opportunities and services that were part of their EAP benefits. The benefits presentation is now part of the onboarding process which ensure all new hires have access to and understand the comprehensive benefits which includes:
-
- Counseling
- Financial Consultations
- Legal Consultations
- Virtual Concierge
- Overall Health and Wellness through a licensed health coach
- Entertainment Discounts
In summary, the RTIC pilot has led to a deeper understanding that we need to prioritize and support our staff’s wellbeing which directly impacts their work with the students. We have moved beyond just talking about being trauma informed to actually being trauma informed by implementing ACEs/CANS-T screenings, using the suggestions from the TRUST-S survey, and focusing on staff development. Our staff retention has increased due to the reinvestment in the classrooms, the increased awareness of ENI services, and the new wellness events hosted for staff. Staff have gained deeper insight into our current practices (TCI and CARE) and their connection to Trauma Informed Care.
RTIC Pilot Case Study: Mothers & Babies Perinatal Network
In March 2021, Mothers & Babies Perinatal Network (M&BPN) was awarded the RTIC Trauma-Informed Care Pilot after a highly competitive review process and began developing a strategy to implement the pilot program and processes a few months later in May 2021.
M&BPN is an experienced provider of maternal/infant and family health and supportive services with a 29-year history of serving south central NY region. Trauma-Informed Care (TIC) is essential because many clients seeking our services have experienced ACEs and various forms of trauma in their past. Through infusing TIC learnings and practices into our work, we hope to foster an environment of compassion, safety, and shared responsibility for both our staff and the individuals that we serve.
The first step for Mothers & Babies was to create their Core Implementation Team (CIT) which included the executive director, the Family Support Services Director, the operations manager, the community health coordinator, and a project manager from Care Compass Network. The CIT team was provided the implementation framework which guided the team through the process of creating a project charter, conducting an initial TRUST organizational self-assessment, evaluating and incorporating staff trainings, integrating TIC practices into policies and procedures, adopting and integrating screenings and interventions into their daily workflow, and incorporating TIC practices into their hiring, onboarding, and retention practices.
Lessons Learned
Throughout the planning and implementation process, the team at Mothers & Babies were faced with many challenges and barriers, one of which was implementing a TIC pilot program in the middle of the COVID-19 pandemic. Despite taking on the pilot project during a difficult time, the team reflected back and recognized how critical and essential the incorporation of this project was to their work, to their staff, and to the people they served.
The pandemic highlighted and reminded them that self-care is essential and not a luxury in order to stay engaged and healthy in their work. The team also discovered that many staff needed different level of support especially with trainings, tools, and resources. By utilizing the staff training evaluations and surveys, Mothers & Babies were able to modify and better understand their team’s needs, opportunities, impacts, and values. They also recognized that proper debriefing time, support, and reflection is critical as staff needed time to digest and truly process the information in the trainings. As a result, the RTIC trainings and program has made a positive impact, thoughtful approaches, and planning among staff and clients.
As the team at Mothers & Babies preserved through these challenging times, the team realized many successes:
-
- Standardization of the ACEs/Trauma screening workflows has increased staff’s comfort and ability in addressing and managing clients and co-workers’ concerns and needs.
- Reflective supervision is practiced during monthly Case Conferences between Community Health Coordinator and Community Health Workers.
- Greater awareness and practice of daily self-care activities, peer support, trauma, resilience, and creation of TIC library to encourage growth mindset.
- Incorporation of the Trauma Informed Care Section in our Personnel Policy Manual helps ensure each new staff are trained and have the appropriate resources and tools needed.
- Completion of individual self-care worksheets during staff meetings has led to better recognition of individual own triggers and what they can do to help themselves.
- Intentional debriefing and reflection time is a MUST after each training/discussion.
The Mothers & Babies CIT embarked on creating and adopting the ACEs (Adverse Childhood Experiences) screening, interventions, and follow-up care policy, procedure, and workflow as part of Milestone 5 requirement. The process required commitment and intentionality from the team. After much consideration, the CIT decided to proceed with piloting the ACEs screening within their community health workers (CHW) program. By taking the time to create, learn and tailor the screening processes and workflows to meet their organization’s needs, the team ensured that the management and communication with clients were delivered in a meaningful and consistent manner across the CHWs. This standardization of the ACEs screening and training resulted in the staff becoming more comfortable with how to address and manage traumas reported by clients and staff.
Through the RTIC Project, the team at Mothers & Babies intentionally engaged with staff to encourage and incorporate self-care and resiliency activities into their day. This recognition on the value of self-care and healing has normalized the conversation and how critical it is to remain effective personally and professionally.
-
- Recognition and value of self-care: Each staff selected a brief activity to incorporate into their daily routine. It is practiced more often than prior to the pilot.
- TIC Staff Resources: Incorporated into our staff onboarding: handouts on self-care breathing exercises, an emergency self-care worksheet, and the ‘Manage Stress’ workbook.
- TIC Library: TIC, resilience, compassion fatigue, self-care, and mindfulness books were purchased with pilot funding to support staff with development and learning.
- Staff Support: Incorporated reflective supervision and daily self-care to minimize the impact of work-related stress.
- Screening Successes: 36 clients were screened in March 2022, of which three were referred for mental health services.
- Intervention Training: Our ACEs Screening team were trained in SPR (Skills in Psychological Recovery).
In summary, the RTIC pilot has led to greater awareness on the impacts of trauma, secondary trauma, compassion fatigue, and self-care resulting in greater prioritization and support for our staff’s wellbeing which directly impacts their work with clients. We have moved beyond just talking about being trauma informed to actually being trauma informed by implementing ACEs screenings, incorporating daily staff self-care strategies, reflective supervision and enhancing our staff’s development by including a Trauma-Informed Care Training Section into our Personnel Onboarding for new hires.
Conclusion
The prevalence and negative impact of ACEs and collective trauma with COVID-19 cannot be overlooked, and in the wake of a global pandemic, we have all been touched by its challenges, difficulties, and stressful experiences physically, socially, emotionally, educationally, and/or economically. Our normal way of life has been disrupted and turned upside down, but we now have the opportunity to change the narrative and reimagine a more compassionate and safe community and environment where each member has a vested interest in its outcomes thus becoming more engaged, contributing in meaningful ways which will ultimately have many positive impacts on the overall health and wellbeing for all.
Implementing TIC isn’t about checking off the box – it’s about taking action, embracing positive role modeling of behaviors, and cultivating an environment of shared common understanding and values. The transformative cultural and mindset shift, operations, and successes of our four (4) RTIC Pilots has affirmed and validated our beliefs in trauma-informed care as a framework to help create and promote a culture that is safe, supportive, and thriving for your staff and team.
Key Takeaways
First and foremost, let’s address the elephant in the room. There were challenges. The biggest of them all was the COVID-19 pandemic. Second was time. Third was limited resources. However, it is important to note that the barriers and challenges reported were similar in nature from across all four pilot settings. They included time, limited resources, competing priorities, CIT’s engagement/participation, staff turnover, and/or organizational leadership. But what was truly unique and amazing was the overall connection and drive towards finding alternatives and methods to advance trauma informed care across their settings given all of the challenges and barriers shared. Each pilot utilized and optimized the framework, resources and tools that were available such as the RTIC program director, RTIC project managers, Action Planning, Weekly CIT touchpoint, Debriefing, and the implementation milestones framework. It did not stop the CIT from pushing forward with their implementation efforts due to the positive feedbacks that were received from their pilot staff and team at the ground level. In sum, it was the greater sense of purpose, need, and value for their staff and team that created the momentum, success, and validation of the Trauma-informed Care program.
Communication is golden. All four RTIC pilots reported that communication is critical especially with adopting, sharing, and training with staff. Being flexible and being agile as a CIT is crucial to advancing, connecting, and embracing trauma-informed care principles and practices with your staff and team. As a result of the RTIC pilot program, each have initiated and expanded upon staff communication strategies, outreach, and incorporating daily and/or regular sharing of trauma-informed responsive approaches and resources to support overall health and wellbeing across their workplace environment. One meaningful adoption was the intentional building in of debrief, reflections, and question time for staff and team especially after discussions and trainings as a result of staff’s feedback from the RTIC Training Evaluation. This helped with teambuilding, communication, connection, safety, supervision, and understanding. Above all, actively listen, acknowledge shared concerns, and respond with compassion and kindness. Ask and don’t make assumptions. Every person just wants to be seen, heard, and belong.
In summary, our RTIC pilot implementation framework has proven its positive benefits, impacts and value as one option to advance and promote a kinder, safer and trauma responsive environment for staff and individual served to heal, recover and thrive. We believe individuals, communities and schools can mobilize and take action in the weeks, months, and years following any community-wide trauma, adversity, or stressors. It is the hope of the RTIC team that lessons learned, successes, and concrete transformations from our RTIC collaboration and the collective meaningful experiences of the pilot program participants, more organizations, schools and healthcare teams will feel empowered and encouraged to create and cultivate a trauma-sensitive environment of their own. Undoubtedly, there will be ongoing and future crises that are likely to occur, which is why proactive planning, implementation, and preparedness is best approached as an iterative, long-term process. One of the lessons learned from our four pilots is to remember that implementing any change takes great intention and patience! It is not a one and done program. Start small and scale up. Communicating and managing a reasonable implementation expectation with leadership, staff, and team will be critical to your team’s health and well-being. Above all else, give yourself and staff compassion and grace.
If you would like to receive a PDF of the full report, please submit a Service Request using the form on the CCN Open Network page.